



In the past 10 years, the decentralized nurse station has gained popularity in new hospital design and construction for several hypothesized benefits: 1) to account for larger nursing unit size with the shift to all-private patient rooms, and reduce walking distance; 2) to place nurses close to the patient bedside, afford more direct patient care time and provide better patient care and 3) to take advantage of the development of health IT and EMR, or electronic medical records, and allow nurses to keep an eye on their charges while charting. However, studies have revealed mixed outcomes of the decentralized nursing unit design. Some showed reduced walking distance and increased patient encounters while others didn’t.
A recent multi-phase and multi-center study conducted by Professors Hui Cai, Kent Spreckelmeyer and Frank Zilm, FAIA, faculty in the Institute for Health and Wellness Design at the University of Kansas School of Architecture & Design, further raised concerns about the impacts of decentralized nursing unit design on patient satisfaction and the communication among nursing teams within the facility.
First phase post-occupancy evaluation findings
During the first phase of the study, the team was contracted by an IHWD affiliate member architecture firm, the Lawrence Group, to complete a post-occupancy evaluation of the newly constructed replacement hospital at SSM Health St. Mary’s Hospital–Jefferson City, Missouri, which shifted from a centralized nursing unit to a decentralized nursing unit design (Fig. 1). The results would give the health system valuable insight before embarking on a renovation of its sister hospital, SSM Health St. Joseph Hospital–Lake Saint Louis, Missouri.

The team evaluated the unit using an Evidence-Based Design checklist promulgated by the Center for Health Design. In addition, the study included a space syntax analysis, which created a heat map of visual connectivity of the layout, patient visibility and peer-to-peer visibility among alcoves.
The team also compared patient satisfaction six months before the move and after occupancy of the new unit. The survey found that all questions about the facility showed a statistically significant increase in score post occupancy. On questions of patient-care quality, most stayed the same, but one dropped slightly, and that was nurses’ response to patient calls. The hypothesis is that due to the physical distance and visual disconnection of decentralized nursing unit design, nurses now have to move farther among the decentralized stations to consult with their peers, perhaps leading to less communication and collaboration, delays in response to patients and patient dissatisfaction.
Second-phase focused study
With the support of the KU New Faculty General Research Fund, Cai has led a group of KU students back to St. Mary’s Hospital to conduct the second-phase study focusing on the impact of decentralized nurse stations on nurses’ communication and teamwork, and thus patients’ satisfaction. During the summer of 2016, adding a second hospital – the University Medical Center of Princeton at Plainsboro, New Jersey – to the data set, the team developed a multistep methodology, which includes focus group interviews and a one-week onsite observation to conduct behavior mapping and tracking of both new nurses and experienced nurses in terms of locations of communication and walking distance.
The research also involves a 30-question, three-part survey that asks nurses about their perception of the unit’s design and the nurse stations in particular, and their perception of teamwork and job satisfaction. The survey results showed that nurses reported limited visibility to other patients and peers, and they found it difficult to locate their peers in the unit and provide timely support to peers with the decentralized layout. It posed challenges for teamwork and implicit learning.
What’s next?
These projects call attention to the innovative, yet untested, design features of decentralized nurse stations. According to Cai, this design trend needs to be further investigated before it is accepted as a standard for every hospital. The key challenge is how to modify the design to achieve the balance between shorter walking distances, better patient surveillance, and retain staff communication, collaboration and learning.
To add to the complexity of the issue, there is a lack of clear definition and classification of what constitutes a decentralized nurse station. There are several variations of nurse station design that combine five basic components: central station, sub-nurse station, pod, distributed alcoves and mobile work stations. However, they are simplified as centralized, decentralized and hybrid nurse station typologies (Fig.2). A lack of consistent standards makes the comparison and evaluation of the decentralized nursing unit even more difficult.
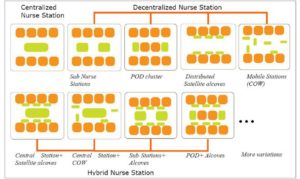
Figure 2: Various types of centralized and decentralized nurse station design. Image courtesy of Hui Cai.
Cai and her team point out the need for more rigorous research to build solid evidence around the decentralized nursing unit design. For instance, it is imperative to develop a comprehensive Evidence-Based Design checklist that allows hospital administrators, designers and facility managers to evaluate many factors that can contribute to the effectiveness of decentralized nursing units. These include nursing unit typology, patient visibility, peer-to-peer visibility, supply and medication locations, supply schedule and information technology. In addition, an expanded study that involves a large number of case studies with various types of decentralized nursing unit layouts will allow cross comparison, and identification of key design characteristics and features on a successful decentralized layout.
A roundtable discussion on the decentralized nursing unit will be led jointly by the University of Kansas and University of Kentucky at the 2017 Healthcare Design Expo + Conference. It will recruit more designers and more hospitals into the discussion. The hope is that the research can lead to design recommendations for alterative models, possibly hybrid, with team bases that have that sense of a small group without losing the close adjacency to patient rooms.