


By Sheila Bosch, Ph.D., LEED AP, EDAC and Jim Kolb, AIA, LEED AP
In 2006, there were more than 119 million visits to emergency departments in the United States. More than half of these visits required the patient to spend more than two hours in the ED receiving care, oftentimes resulting in prolonged wait times for treatment due to overcrowding. During these times, conditions in the ED are often chaotic, noisy and may contribute to confusion, distraction and mistakes.
In this era of increased numbers of uninsured and underinsured patients, reductions in reimbursement and increased liability, healthcare providers are under pressure to improve productivity and the quality of outcomes. With increasing frequency patient volumes are exceeding existing ED capacity. Staffs across the country have worked to increase capacity, in part through process redesign, as demonstrated in the Culp and Jarvis article in the January/February issue of Medical Construction and Design. These process improvement strategies may be deployed with or without capital improvements and are typically a cornerstone of an ED quality assurance program. There is increasing evidence that healthcare processes are inextricably linked with physical space.
Gresham, Smith and Partners conducted a survey aimed at understanding the prevalence of process improvement strategies within the ED setting, while also capturing data regarding the perceived physical conditions of the EDs surveyed. A survey tool was developed and pilot tested. In-person, structured interviews were conducted using the survey tool for approximately half of the surveys, and included tours of the emergency departments. To increase the sample size, the survey was sent to ED directors across the country. The total number of completed surveys was 48.
 The majority of respondents represent urban hospitals (45 percent), followed by suburban (40 percent) and then rural (15 percent), most of which are not-for-profit (78 percent). Participants were located in at least online casino 18 different states (note: not all participants included their location) and represent both teaching (59 percent) and non-teaching hospitals (41 percent). One free-standing ED responded to the survey. The sample includes community (47 percent), tertiary (40 percent) and quaternary hospitals (13 percent), as well as trauma centers (43 percent) and those that are not (57 percent).
The majority of respondents represent urban hospitals (45 percent), followed by suburban (40 percent) and then rural (15 percent), most of which are not-for-profit (78 percent). Participants were located in at least online casino 18 different states (note: not all participants included their location) and represent both teaching (59 percent) and non-teaching hospitals (41 percent). One free-standing ED responded to the survey. The sample includes community (47 percent), tertiary (40 percent) and quaternary hospitals (13 percent), as well as trauma centers (43 percent) and those that are not (57 percent).
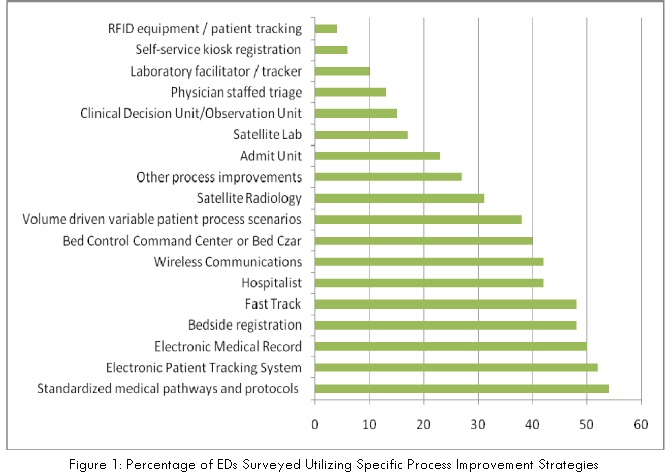
Respondents were asked whether or not they have implemented one or more of several specific process improvement strategies: bedside registration, kiosk registration, physician staffed triage, standardized medical pathways and protocols, volume driven variable patient process scenarios, bed control command center, clinical decision unit, nursing unit hospitalist, electronic medical records, electronic patient tracking dashboard, wireless communications, RFID equipment/patient tracking, laboratory facilitator/tracker, satellite lab, satellite radiology, admit unit, and fast track. 
Figure 1 demonstrates the percentage of respondents who have implemented each of these process efficiency improvements. Additional strategies were also identified, and include referring non-emergent patients to other community providers (after a medical screening) or treating them at a specified cost, creating a temporary pre-admission holding area outside of the ED, afterhours use of the surgery out-patient nursing unit as a staging area for patients who were to be admitted, and an ambulance triage function to unload, triage and hold ambulance patients. The majority of respondents (Figure 2) indicated they have observed measurable improvements as a result of implementing process-improvement strategies.
Sheila Bosch, GS&P’s director of research, serves as a firm-wide resource for planners and designers as they apply research evidence to enhance quality, safety and efficiency in healthcare settings. Sheila also contributes to this important field of evidence-based design by conducting original research aimed at understanding how the physical environment affects health and performance outcomes. She can be reached at sheila_bosch@gspnet.com.
Jim Kolb has designed more than $400 million in architecture for healthcare. A proponent of Evidence-Based Design, he incorporates elements into his designs that have improved medical outcomes. He can be reached at jim_kolb@gspnet.com.
