
Subscribe Now






Discrete Event Simulation: Enhancing Flow in Healthcare Design
By Noah Tolson and Jim Cain
Discrete event simulation, or DES, which has been utilized across industries for several decades, provides a virtual environment to track and visualize patients, equipment and providers as they move through the steps of care. It is an important tool in supporting Lean design in the healthcare environment.
 In order to achieve the desired physical environment, healthcare architects rely on a vast amount of data — and the tools for harnessing that data are becoming more advanced. Just as BIM optimizes early decision-making in the design phase, DES can influence the design of workflow and patient flow prior to construction.
In order to achieve the desired physical environment, healthcare architects rely on a vast amount of data — and the tools for harnessing that data are becoming more advanced. Just as BIM optimizes early decision-making in the design phase, DES can influence the design of workflow and patient flow prior to construction.
This virtual environment provides the ability to test a multitude of ‘what if’ scenarios with clients to understand the impact that different layouts have on workflow, patient flow and resource utilization. The result is an increased confidence that the design will support current needs, as well as provide insight on incorporating flexibility into the design to accommodate inevitable future changes.
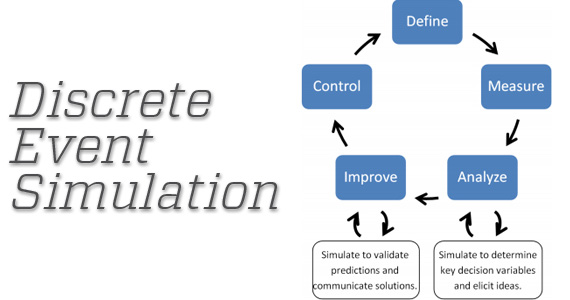
DES provides three key advantages over other methods of analysis:
- Real live variability can be applied to a critical key measurement, such as patient demand, times to complete key tasks, wait times for key resources or simply waiting for care, etc.
- Naturally occurring constraints exist when the demand for services/resources exceeds capacity. DES models allow constraints to be included by identifying the interdependencies between resources available and resources required.
- DES models simulate the passing of time (into the future) and record key metrics such as wait times, processing times, resource utilization and equipment utilization as they relate to varying patient demand and varying patient acuity. This helps with the daunting task of attempting to predict when the care is to be provided and by whom.
Utilizing Lean design, architectural teams appropriately spend time observing and recording workflow and patient flow to document and understand the current state. Accurately predicting the future-state workflow and patient flow has always been difficult to project and arrive at consensus because workflow analysis has traditionally been based on averages. While averages are a good place to start, they don’t tell the entire story.
This is where DES, due to the advantages described above, is highly valuable. Using a DES tool to model the various hospital processes in the new structure provides much more insight into the effectiveness of potential designs. DES helps evaluate the workflow, resources and patient demand more realistically and simultaneously, which allows healthcare decision-makers to be more confident in the design solutions.
Case Study
A DES model was recently used to help one healthcare organization evaluate a newly constructed 220,000-square-foot outpatient facility. The facility was intended to centralize the services of affiliated specialty practices and education and research centers. This five-floor clinic would allow 65 providers from 13 different practices throughout a specific region to converge in one patient-friendly location. Quality and service was expected to increase greatly by having referring physicians in one collaborative environment. Spreadsheet models were initially used to study the consolidation and facility design project, but provided only static information that relied heavily on the use of averages.
This made it hard to accurately study the many complex processes that occur continuously in an outpatient setting. With limited data available, physicians and administration had difficulty reaching consensus on space requirements and efficient room utilization. Using DES, a solution proposed first- and third-floor designs of the clinic in order to analyze capacity and resources against the current data on patient flow from all the converging practices. The simulation examined the individual practices over a five-day period (Monday-Friday) during regular business hours. The measuring criteria consisted of the following:
- Exam room utilization
- Physician and staff utilization
- Number of patients at check-in
- Time spent in check-in queue
- Patient activity times
- Number of patients in imaging queue
After multiple scenarios were run, the output data confirmed there would be sufficient room for the consolidation of practices on the first and third floors. In fact, the analysis showed that on certain days of the week there were not enough providers to fill the capacity on those two floors.
This is one example that illustrated the advantages of DES. Similar methods have been used to more accurately project operational outcomes and compare design solutions.
Author: Noah Tolson and Jim Cain
Noah Tolson is a principal and the practice area leader for planning with Array Architects and may be reached at ntolson@array-architects.com. Jim Cain, MSN, is the director of healthcare solutions with ProModel Corporation and may be reached at jcain@promodel.com.
Posted November 11, 2013
More Articles:
- CxA Workshop & Exam
Apr 29, 2024 – Apr 30, 2024 - EMP Seminar & Exam at CxEnergy 2024
Apr 29, 2024 – Apr 30, 2024 - CxEnergy
Apr 29, 2024 – May 2, 2024 - PHCC West 2024
Apr 29, 2024 – May 2, 2024 - Lean in Design Forum 2024
May 1, 2024 – May 2, 2024 - IFMA’s Facility Fusion Conference & Expo
May 5, 2024 – May 7, 2024 - ASHE Academy 2024
May 6, 2024 – May 10, 2024

