


 By Bhargav Goswami and Ellen Barrington
By Bhargav Goswami and Ellen Barrington
The U.S. population is aging, with 12 percent of citizens currently over the age of 65, and this number is growing. Hospitals are seeing more elderly patients, with 35 percent of all hospital stays on average attributed to those over age 65. In addition, 36-58 percent of these older adult patients suffer iatrogenic illness (adverse affects from being in the hospital) during a stay, with many common complications being both preventable and treatable.
While the vital components of a healing environment remain valid for older patients, these issues are compounded by geriatric patients’ particular vulnerabilities. Older patients present hospitals with a unique set of concerns, including co-morbidities, chronic illnesses, cognitive and psychiatric needs, problems with activities of daily living, or ADL , sensory issues and the need for socialization. All concerns are different from those of younger adult patients.
By focusing on critical design features that evidence has shown to facilitate better outcomes, those creating the spaces can make healthcare environments that not only improve patient safety, but also protect functional abilities and promote socialization.
Areas of particular focus include:
- Activity: Older patients need adequate room and support for ADLs
- Socialization: Older patients benefit from space designed to encourage social interaction
- Attention from clinical staff: Environments should improve caregivers’ efficiency and allow time for additional care and increased interaction with
 elderly patients
elderly patients - Lighting: Those suffering from a decline in visual acuity benefit from proper lighting conditions (i.e., uplighting, glare reduction, natural light and shades)
- Bathrooms: Patient toilets with non-slip flooring, grab bars and space for roll- ins, etc., aid access and self care
Case Study: Ocean Medical Center’s Acute Care for the Elderly Unit
Ocean Medical Center in Brick, N.J. is one of a select few hospitals in the country that has an inpatient unit designated for the Acute Care of the Elderly, a model of inpatient care geared toward avoiding complications and returning elderly patients to a level of baseline function prior to hospitalization through attention to staffing, care protocols and the unit’s physical design.
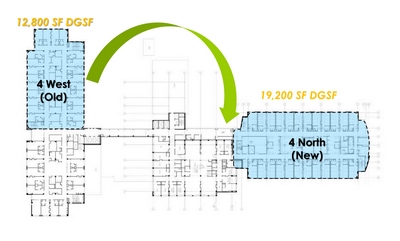
A planned move of the 40-bed ACE unit to a larger shelled floor plate presented an opportunity to use Evidence-Based Design principles to address issues specific to elderly patients, such as increasing safety, reducing falls, improving wayfinding and increasing ambulation and social interaction. The design team included nurse advocates in all aspects of the design process that were able to promote the goals and priorities of the project, and inform and represent patient constituents.
Among the important considerations was the need to ambulate patients; the design of the new unit supports the out-of-bed program. Evidence suggests functional decline in older adults admitted to hospitals is a major predictor of outcomes and that decline can occur in as little as day two of hospitalization. Design concepts employed include: spacious rooms with geriatric chairs at patient bedsides for the out-of-bed program, an activity room with games, era-appropriate music and a kitchen area, easy to read signage and floor patterns marked to indicate walking distances and large entrances to rooms to support ambulation.
 Other concepts to improve patient safety include providing all accessible patient toilets with grab bars on either side of toilets, accessible showers with benches and rubber flooring. The lighting throughout the unit reduces glare and improves visual acuity with a mix of natural light, uplighting, shades and non-glare flooring.
Other concepts to improve patient safety include providing all accessible patient toilets with grab bars on either side of toilets, accessible showers with benches and rubber flooring. The lighting throughout the unit reduces glare and improves visual acuity with a mix of natural light, uplighting, shades and non-glare flooring.
A critical improvement in the redesign was the decision to move to decentralized nursing stations equipped with necessary supplies (meds, linens, etc.), which reduces nurses’ travel distances and times while it increases an ability to provide direct care and reduces response time in the case of patient distress.
Post-occupancy evaluations of the unit as well as Press Ganey and Gallup Scores comparing the old and new units reveal improvement not just in perception of care. Analysis of the data shows marked decline in the number of falls, injury severity and nosocomial wounds. It also shows actual improvement in out-of-bed rates and discharges.
The ACE unit is a promising example of the benefits of using Evidence-Based Design as part of a geriatric initiative.
Bhargav Goswami, AIA, LEED AP, is principal at WHR Architects.
Ellen Barrington, MSN, RN-BC, NEA-BC, is senior manager of Patient Care Services at Meridian Health.
