


Flow Path of Air Matters in Patient Rooms
Air is the primary carrier of heat, moisture, contaminants and airborne pathogens in healthcare facilities such as patient rooms, isolation rooms and operating rooms. Recommended flow rate of supply air or number of air changes per hour are developed by considering only the overall dilution of the contaminants in the exhaust air streams. However, the flow path of supply air and how it is distributed is important in understanding the distribution of heat and contaminants within the space.
The flow path of supply air determines thermal comfort, air quality and potential for transmission of airborne pathogens in the patient room. Airflow patterns within a patient room can depend on several factors, including the location and type of supply diffusers, supply airflow rates (air change rates) and associated diffuser throws, supply air temperature, size and locations of room return, bathroom exhaust flow rates, locations and strengths of various heat sources in a room, arrangement of furniture and other obstructions to airflow and relative location of a patient in the room.
Visualization of airflow patterns and real-life evaluation and testing all the parameters that affect the airflow distribution is time consuming and labor intensive, if not impossible. In such situations, computational fluid dynamics simulations become an attractive alternative to analyze and optimize the performance of HVAC system configuration with real-life scenarios. CFD has been widely employed in the design and optimization of various products and processes in a variety of industries ranging from aerospace, automotive to chemical and biomedical. CFD is based on scientific laws of physics related to transport of fluid, heat and mass within a space.
CFD simulations help in visualization of airflow patterns, temperature distribution, concentration of contaminants and flow path of airborne pathogens in a 3-D space. CFD analyses provide valuable insights, which help in improving the designs and in developing mitigation strategies in the case of problem resolution.
Virtual Patient Room
In a recent study, a virtual patient room was created with the help of CFD simulation to understand how the location of a return grill in a patient room can affect the airflow patterns, temperature distribution and the probable flow path of airborne pathogens. The 3-D CFD model of a patient room included a patient, a caretaker, seating area, door to the corridor, door to the bathroom and supply and return air locations (figure 1). This analysis was performed for two different HVAC configurations – one near the room door and the other over the patient’s head. The room contains heat-generating equipment including lighting, monitor, infusion pump, television, computer and two occupants – the patient and the caretaker.
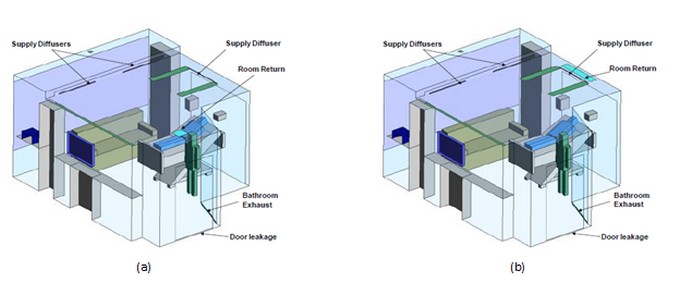
a) Case 1: room return is located near the door
b) Case 2: room return moved behind the supply diffuser
Figure 1: Schematic diagram of CFD models for the analysis of a patient room showing two different locations for the return grill.
The air is supplied through three single-slot linear diffusers. The two linear diffusers placed on the drop ceiling are directed toward the window to account for the solar heat gain from the window. The linear diffuser over the patient is designed to supply air at an angle directed toward the room. The room was assumed to operate under slightly negative pressure with the exhaust flow from the bathroom exhaust fan. The probable flow paths of airborne pathogens are analyzed by tracking the path of air streams emerging from the patient’s face.
Valuable Insights
These analyses provided valuable insights into the 3-D airflow patterns, temperature distribution and the resulting thermal comfort and, importantly, the probable flow path of airborne pathogens. Thermal comfort of occupants was analyzed by employing predicted mean vote index as described in ASHRAE 55 standard for thermal comfort. As mentioned before, two cases were analyzed for two different locations of the return air grill.
In the case 1 analysis, the linear supply diffuser is located right above the patient’s head and the return grill is located near the door. The exiting air jet from the supply diffuser forms a strong recirculating pattern over the patient and behind the bed. As a result, the air flows upward over the patient and gets entrained back into the supply air stream (figure 2a). As shown in figure 2b, this re-circulation creates a slightly higher air temperature near the patient’s head. Figure 2c shows the distribution of the PMV, the thermal comfort index, which varies from -3 (too cold) to +3 (too hot). PMV values of 0 indicate a thermally comfortable environment, which is indicated by the green color in figure 2c. As shown in this figure, at the 4-foot height from the floor, the occupant thermal comfort is at neutral level (PMV close to 0.0). However, the airborne pathogens releasing from the patient’s face can get pulled into the supply air stream and eventually spread into the entire room (figure 2d). It shows the supply diffuser becomes a vehicle to entrain and spread the pathogens into the room.
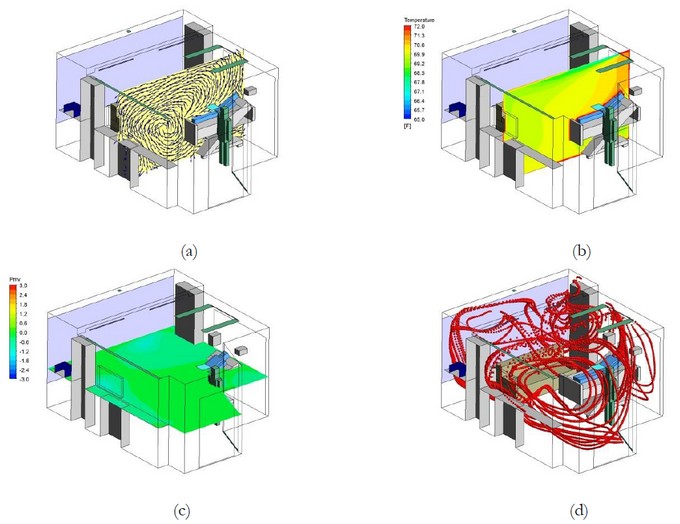
Figure 2: Results for the case 1 analysis showing a) airflow patterns, b) temperature distribution, c) PMV distribution at 4-foot height and d) resulting flow path lines indicating probable trajectory of airborne particles released from the patient’s face. It shows even though patients and other occupants can be the thermally comfortable in the space, the airflow patterns in the room can spread the airborne pathogens released from patient’s face into the entire room.
Ideally, the supply air from the diffusers should pass over the patient and return back to the return grill in a single pass without mixing into the supply stream and without recirculating into the room. The modifications in the HVAC configuration of case 2 attempts to achieve this. For the case 2 analysis, the size of the return grill is increased and moved behind the supply diffuser over the patient’s head (figure 1b). Relocation of the return grill right behind the supply diffuser provides ready access for the return air to exit from the room without significant re-circulation.
 Figure 3: Results for case 2: room return moved behind the supply diffuser showing a) airflow patterns, b) temperature distribution, c) PMV distribution at 4-foot height and d) resulting trajectory of airborne particles released from the patient’s face. It shows simple modifications in the HVAC configuration without changing air change rates can significantly improve the airflow patterns and resulting flow path of airborne pathogens without affecting the thermal comfort of occupants.
Figure 3: Results for case 2: room return moved behind the supply diffuser showing a) airflow patterns, b) temperature distribution, c) PMV distribution at 4-foot height and d) resulting trajectory of airborne particles released from the patient’s face. It shows simple modifications in the HVAC configuration without changing air change rates can significantly improve the airflow patterns and resulting flow path of airborne pathogens without affecting the thermal comfort of occupants.
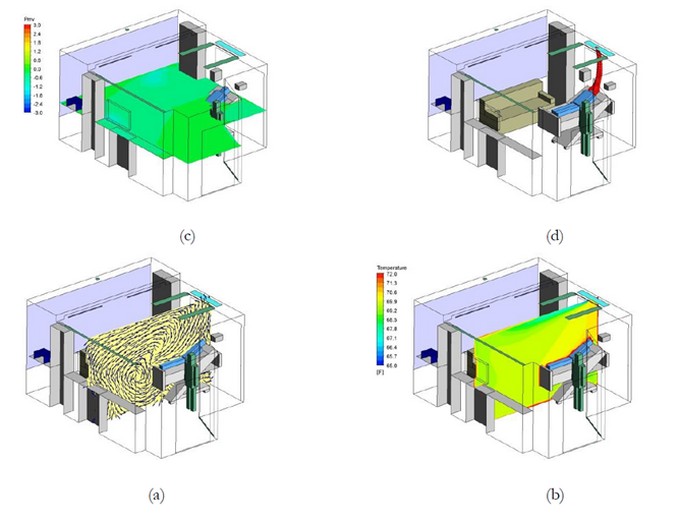
Such modification does not significantly affect the temperature distribution and resulting thermal comfort of occupants, but it significantly modifies the flow path of the return air and the airborne particles (figure 3). In this case, the supply air still moves over the patient but does not get pulled back into the supply air stream. The return air carrying airborne pathogens can readily exit the room without re-circulation. It clearly shows such simple modification in the HVAC configuration can potentially provide a single flow pass over the patient and can provide a cleaner environment, reduce the probability of entrainment of the airborne particles back into the supply air stream and can avoid the spreading of airborne pathogens in the room.
A virtual patient room was created with the help of CFD models to evaluate the impact of return grill location on the flow path of airborne pathogens. These analyses provided valuable insights into airflow patterns, temperature distribution, thermal comfort of occupants and, importantly, on the probable path of airborne particles (pathogens) in a patient room. The traditional HVAC configuration of placing the return grill near the room door can potentially pull the airborne pathogens released from the patient’s face back into the supply air stream and can eventually spread those into the entire room. However, a simple modification of placing the room return right behind the linear supply diffuser over the patient’s head can potentially create a cleaner environment by providing an easy pathway to airborne pathogens into the return grill, which can avoid re-circulation of contaminated air back into the room.
It should be noted, a combination of locations and type of supply diffusers, locations of the room return and supply airflow rates can affect the airflow patterns, which are quite complex and specific to a particular design configuration. Therefore, it is difficult reach to any general conclusions about the optimized design configuration and placement of supply diffusers and return grills in a patient room. However, this study demonstrates CFD analysis can be an effective tool in gaining insight and optimizing the design of air distribution systems in healthcare faculties. Such efforts can help in designing patient rooms with better occupant thermal comfort along with the best possible hygienic conditions.
Editor’s Note: This article was based on “Role of HVAC System Configuration on Probable Flow Path of Airborne Pathogens in a Patient Room,” a paper presented during ASHRAE’s annual conference held in Denver, Colorado. An abbreviated version of this article appeared in the July/August issue of MCD magazine.
